

What if we had used the RT-PCR test from the (2003) original SARS-CoV-1 as our covid test?
Using RT-qPCR tests with false-positive results to evaluate the endpoint in COVID19 vaccine development might have artificially inflated the vaccine effectiveness.

Today I am spotlighting the work of American pathologist Dr Sin Hang Lee whose empirical data from testing the PCR test raises multiple issues.
I will highlight parts of his papers in an attempt to tell the story:
An important point here is that you can perform routine nested RT-PCR testing followed by DNA sequencing to “to verify the authenticity of the amplified product.”
In 2020, Dr Lee did just that and published his findings in the International Journal of Geriatrics and Rehabilitation:
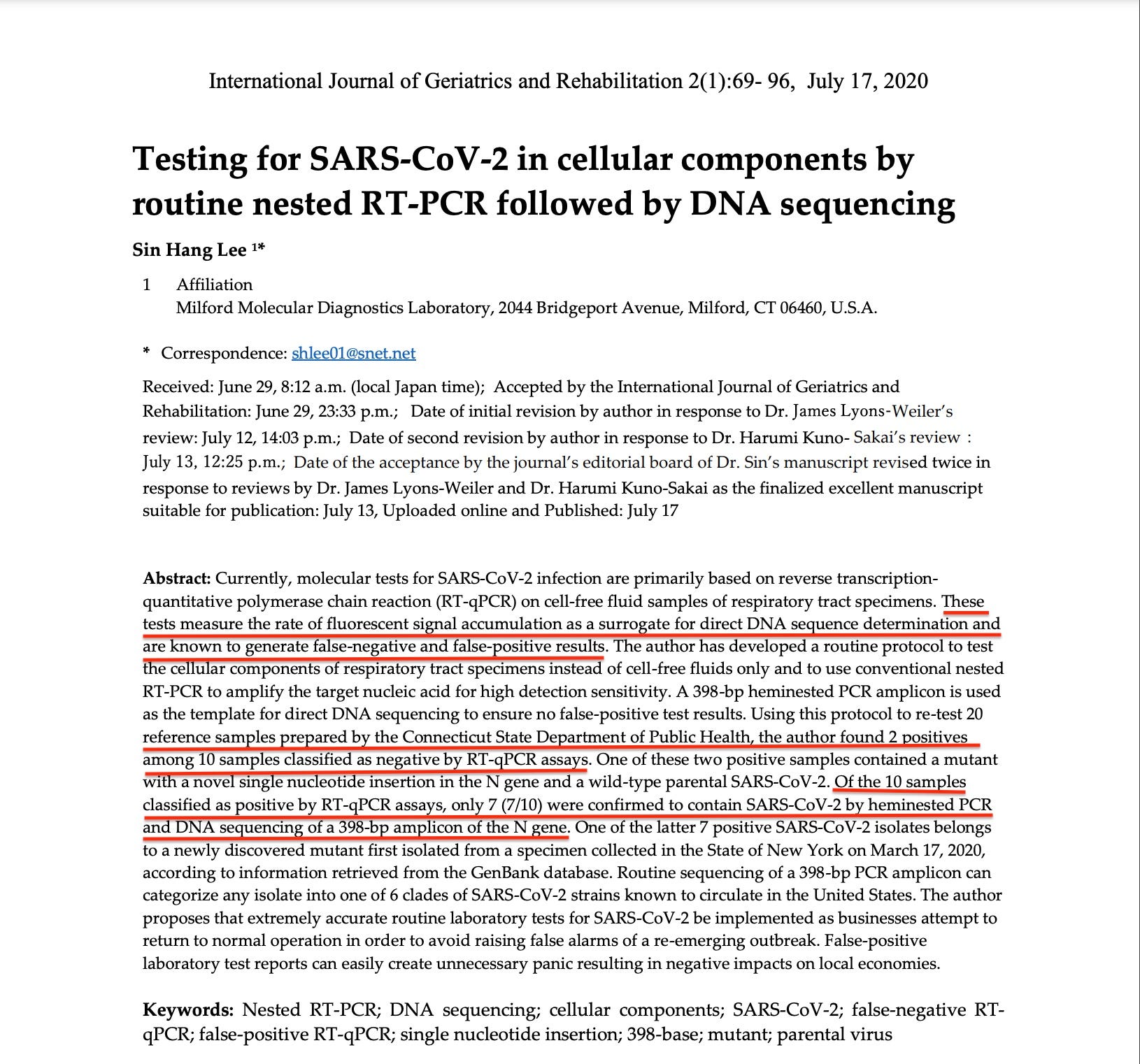
So Dr Sin HangLee found serious issues with the results of the tests classified as positive ( and negative) by RT-qPCR assays ( the so called qPCR assays used unvalidated CT cut-off thresholds):
Contrary to the previously established protocol and guideline set by the CDC and the FDA for the diagnosis of SARS-CoV-1 and for RNA viruses, the SARS-CoV-2 commercial RT-qPCR assay kits are generating a Ct number, an unproven surrogate for nucleotide sequence, for “the presumptive qualitative detection of nucleic acid from the 2019- nCoV” under emergency use authorization [14].
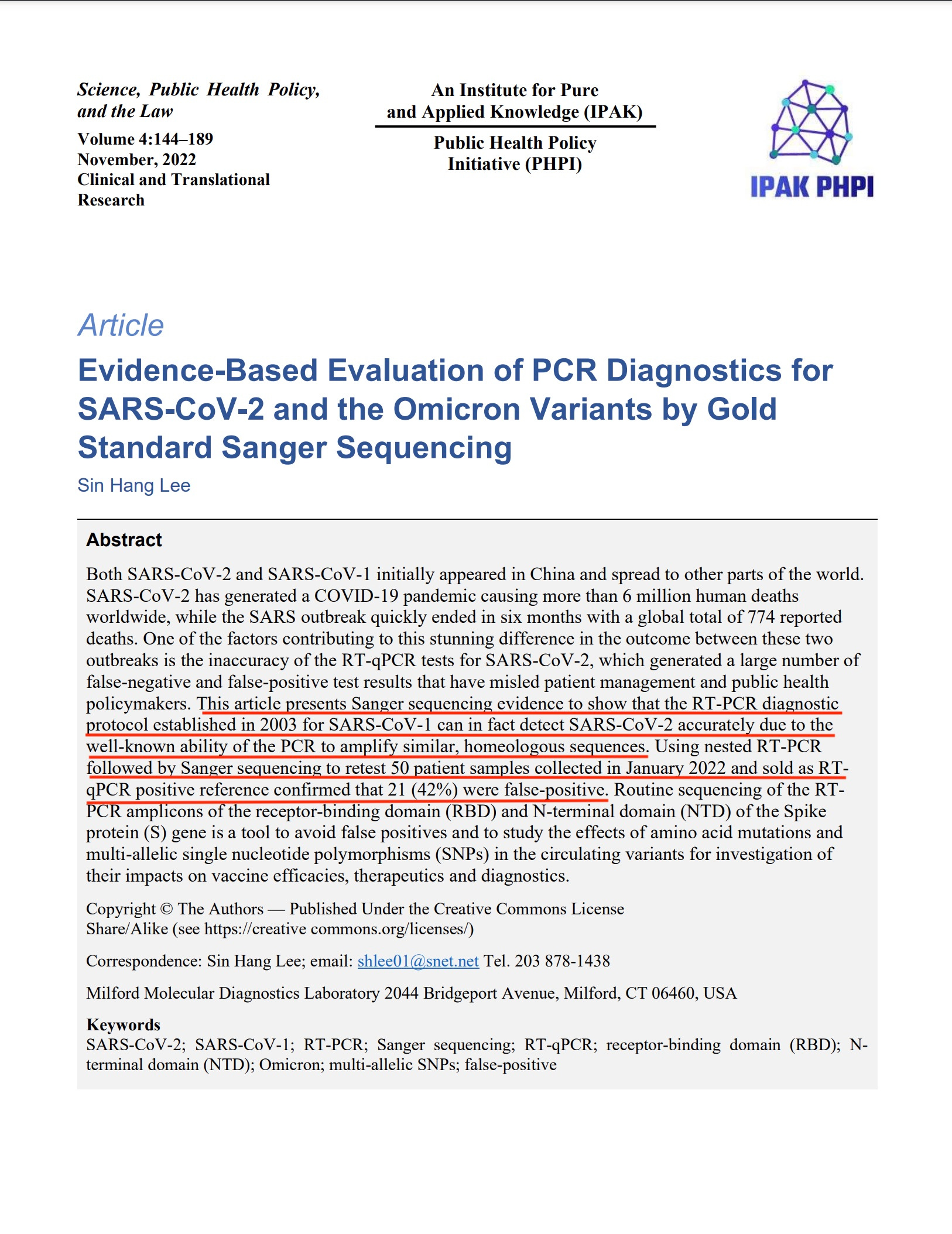
Using conventional RT-PCR and Sanger sequencing, as recommended by the CDC for SARS-CoV-1 in 2003, to retest two sets of patient samples showed that the current commercial RT-qPCR test kits for SARS-CoV-2 assays generated at least 20% false-negative and 30% false-positive results on nasopharyngeal swab samples collected from patients with respiratory infection in early 2020 [15] and 47% false positives in the nasopharyngeal swab samples collected from patients with respiratory infection in the month of October, 2020 in the United States [16], before any variants of concern emerged.
The SARS outbreak was eradicated in July 2003 with a global total of 8,098 reported cases and 774 deaths.
An important contributor to the successful eradication of SARS 1 was accurate testing.
Apparently back then, pathologists & the CDC knew, how to use RT-PCR,
how shall I put it, mindfully.
The present study has presented experimental evidence to support the claim that the world could have taken advantage of the partially specific nature of PCR amplification by using the CDC-recommended SARS-CoV-1 specific RTPCR primers and diagnostic protocol [10] for accurate detection of SARS-CoV-2 at the early stage of the COVID-19 outbreak to avoid or to curtail a pandemic and to lower the death toll.
The flaw of the RT-qPCR as a diagnostic assay is that it depends on a number, which may vary from laboratory to laboratory and from test run to test run, to distinguish between the positives and the negatives of a test result
Using qPCR for the diagnosis of infectious diseases, such as Monkeypox virus infections, the CDC requires the testing laboratories to establish their own positive control Ct cut-off value or to prepare a standard curve in order to identify the samples that are truly positive for Monkeypox virus DNAs [51]. However, no such requirement is set for the SARS-CoV-2 RT-qPCR assays [52].
However, when qPCR is adapted into a “plus/minus” or a “yes/no” assay for the purpose of detecting genomic DNA of an infectious agent in a complex clinical specimen, it needs to distinguish zero from nonzero in a standard curve.
these points are important:
As a result, the diagnostic laboratories do not have a validated quantitative standard curve or a verified Ct cut-off value for SARS-CoV-2 RT-qPCR tests; cut-off values differ from laboratory to laboratory. In some circumstances, the distinction between background noise and actual presence of the target virus is difficult to ascertain [53] in these RT-qPCR assays; a 42% false discovery rate in SARS-CoV-2 RT-qPCR assays is not unexpected. The need for a confirmatory test with 100% specificity was already recognized by the current CDC director 2 years ago [54].
Using RT-qPCR tests with false-positive results to evaluate the endpoint in COVID19 vaccine development might have artificially inflated the vaccine effectiveness.
For example, the COVID-19 vaccine efficacy in the clinical trials was primarily assessed by the results of RT-qPCR testing of placebo participants with minor symptoms[55].
Without confirmatory Sanger sequencing of the RT-qPCR products, the claim of the BNT162b2 vaccine being 95% effective against COVID-19 [56] becomes questionable.
The SARS-CoV-2 virus that causes the COVID-19 pandemic is genetically closely related to the SARS-CoV-1 virus that caused the outbreak of severe acute respiratory syndrome (SARS) in late 2002. Both viruses have a genome of single stranded positive-sense RNA of nearly 30,000 nucleotides that share a 79% similarity [1,2], and both use the angiotensin-converting enzyme 2 (ACE2) as their major receptor to enter the host cell [3].
The public record shows that during the 2002/2003 SARS outbreak in China, the laboratory diagnostics for SARS cases were based on conventional RT-PCR using a series of primers.
“After purification of the PCR products, cycling sequencing reactions were performed to determine the nucleotide sequence for the definitive molecular diagnosis of SARS-CoV-1 infections” [8].
“According to one report, the US CDC-designed PCR primers were directed to the polymerase gene of all coronaviruses and amplified a 405 bp fragment from the newly emerging coronavirus. The amplicon was then sequenced and compared with the GenBank reference sequences for molecular diagnosis [9]”.
“In another document, the CDC recommended using three specific primers to perform RT-PCR on patient samples and to sequence a 348-bp PCR amplicon “to verify the authenticity of the amplified product””[10].
It seems when it came to new SARS, vs old SARS, it was all about this new commercial testing based on cycle thresholds (qPCR).
For some reason, when it came to “new SARS” aka SARS-CoV-2 vs “old SARS” or SARS-CoV-1 our authorities focused on the new commercial test, the “current thing” in testing, without verifying the “authenticity of the amplified product” which left us with a flawed test, waiting to be exploited by a flawed system, run by flawed people.
************************************************************************************************************
Please become a supporter of my work:
buymeacoffee.com/LkRNpg8ydW
or my freedom QR code:

Dr. Paul - I wonder if you've seen the recent video with Dr. McCullough & Dr. Aseem Malhotra, sponsored by the U.S. VSRF group? It's only 4 minutes long. Dynamite! All about the "died suddenly" phenomenon. Cardiac arrests. I'm sharing it widely right now. (It was published on Nov. 4th but I only saw it today.) https://rumble.com/v1rl1kk-until-proven-otherwise-featuring-cardiologists-dr.-peter-mccullough-dr.-ase.html?utm_source=substack&utm_medium=email (I'm from Canada, where, as you know, 80 MDs have died in recent months.)
Hi Paul. I’d like to interview you for an article on vaccine related gynecological issues/falling birth rates. Can you email me at marybethpf@aol.com? Mary Beth Pfeiffer
https://www.thefirstepidemic.com/new-index