

Hospital acquired infections . . . why aren't we testing and treating for vit D ?
From JAMA Surgery 2014 (BC), another reason to like vit D.

I was reading this 8 year old paper in JAMA Surg and I know how much hospital administrators hate hospital acquired infections. What with the catheter-related urinary tract infections (CRUTIs) are the most common HAI (Hospital Acquired Infection) in the United States, surgical site infections (SSIs), pneumonias, and bloodstream infections are all significant causes of HAI’s
“Hospital-acquired infections (HAIs) are a major source of nosocomial morbidity and mortality. Approximately 10% to 13% of all hospitalized patients in the United States develop HAIs, which translates to an annual incidence of roughly 2 million new cases and almost 100 000 potentially avoidable deaths per year. Excess annual health care expenditures attributable to HAIs range from $28 billion to $45 billion,6 and the average hospital length of stay is prolonged by 5 to 9 days in patients who develop a nosocomial infection.”
Ok, so a potential 100,000 avoidable deaths and billions of dollars at stake, you’d think this might be on someones radar?
“However, it is important to note that aside from the use of neuraxial anesthesia, all existing strategies to minimize HAIs look to modify factors external to the host. Moreover, to our knowledge, few studies have looked at methods of optimizing natural host responses to infection in the perioperative setting.”
“Recently, the immune-modulating effects of vitamin D have received significant attention. Indeed, a role for vitamin D in the prevention of HAIs has been suggested. However, to date, the influence of vitamin D status on surgical outcomes is largely unknown”.
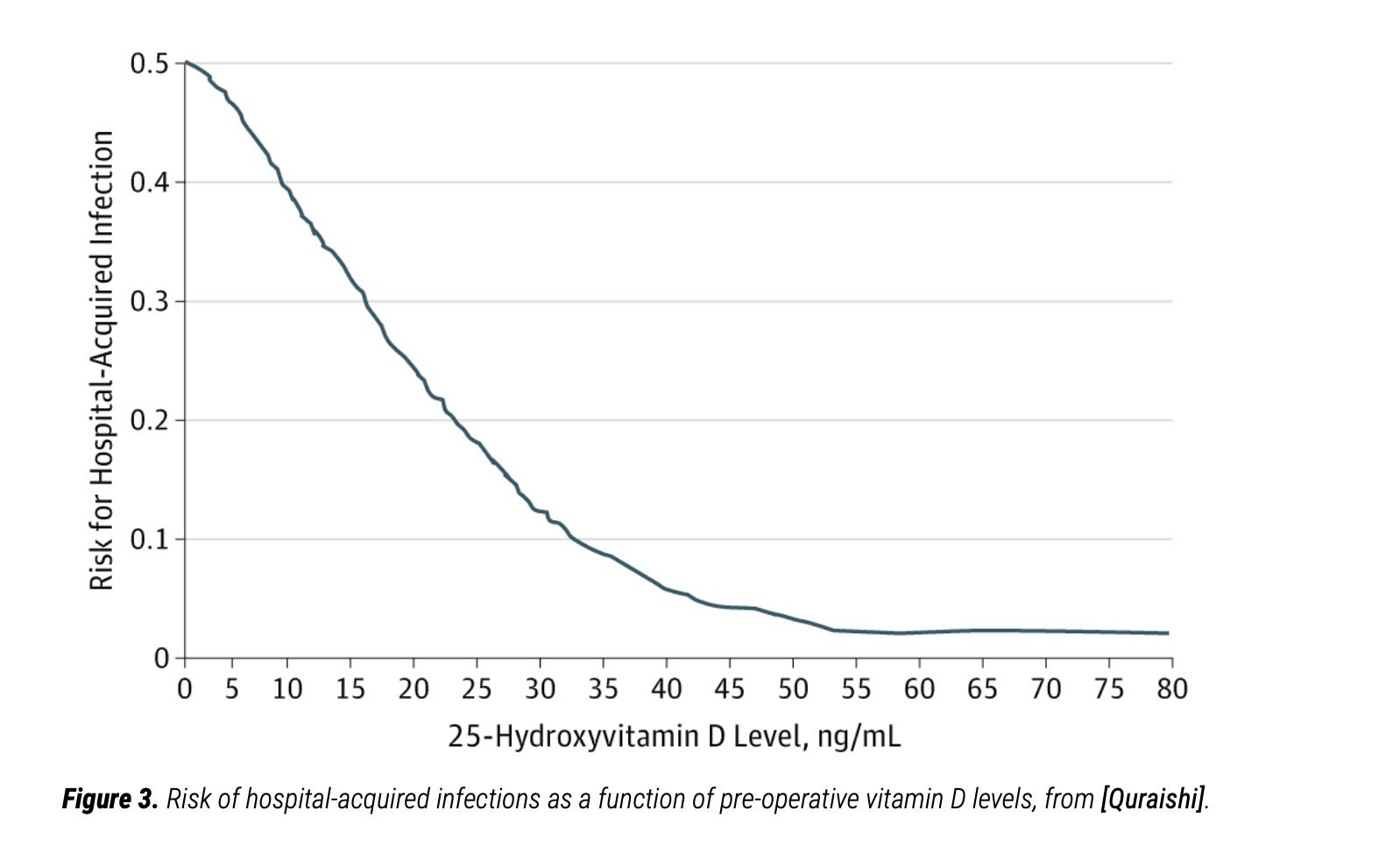
What they found in their obese population of patients, you know, the same population that have a hard time with covid, who were set up with all the co-morbidities that made people vulnerable to covid … was a 3 fold reduction, just comparing those below, and those above 30 ng/ml.
Now one more section that caught my eye:
“Recent studies have demonstrated that cells of the innate and adaptive immune system express the vitamin D receptor and respond to stimulation by 1,25-dihydroxyvitamin D, the hormonally active vitamin D metabolite. Also, 1,25-dihydroxyvitamin D is important for the interferon-γ–dependent T-cell response to infection. Moreover, 25(OH)D links toll-like receptor activation and innate immunity, upregulating expression of the antimicrobial peptides cathelicidin (LL-37) and β-defensin. In humans, LL-37 has been shown to have potent activity against bacteria, viruses, fungi, and mycobacteria, and it is highly expressed at barrier sites. As such, LL-37 may provide important first-line defense mechanisms for the innate immune system. Prospective studies by members of our research group and others have shown maximal LL-37 expression to occur at 25(OH)D levels between 30 and 35 ng/mL, thereby strengthening the biological basis for the association between higher 25(OH)D levels and optimal immune function.”
I mean low hanging fruit, hello, anybody out there?

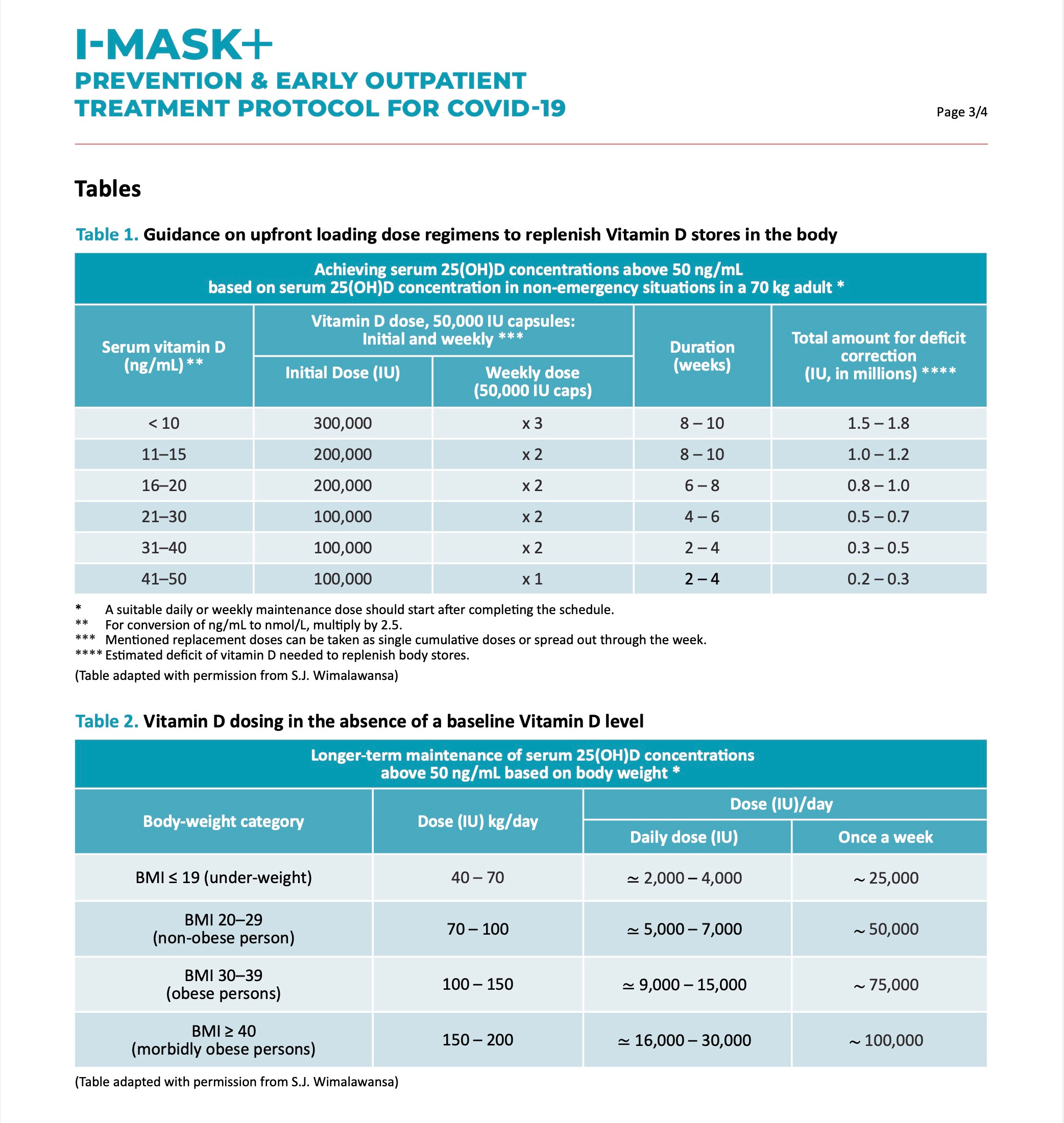
Notice it works best as part of early treatment (doesn’t everything?) but still has benefit in late disease and as prophylaxis … not many treatments you can say that about (Ivermectin is another).
Look to places like the FLCCC.net. e.g. I-Mask protocol to get their latest thinking on vit D dosing : It’s likely more than you have been thinking.
Please see the research articles cited at "What every MD, immunologist, virologist and epidemiologist should know about vitamin D and the immune system": https://vitamindstopscovid.info/05-mds/ . These start with Quraishi et al. 2014, which you cite above. If doctors all over the world had been properly interested in nutrition, this article would be known to them all by now and the graph would be framed and displayed prominently in doctors' waiting rooms all over the world.
Unfortunatly, most doctors have no understanding of vitamin D's importance to the immune system, or at best a vague idea about it, but without understanding that it is the circulating 25(OH)D the immune cells need, and that the very low level of hormonal 1,25(OH)2D for calcium-phosphate-bone health has no effect on the immune system: https://vitamindstopscovid.info/02-autocrine/#02-nothorm .
For early treatment of COVID-19, sepsis, MIS-C etc. a single oral dose of 0.014 mg calcifediol (which is 25(OH)D) per kg bodyweight raises ciculating 25(OH)D (in general) safely over 50 ng/mL 125 nmol/L in 4 hours. See the FLCCC's MATH+ protocol https://covid19criticalcare.com/covid-19-protocols/math-plus-protocol/ for this, on Prof. Sunil Wimalawansa's recommendation - and: https://vitamindstopscovid.info/04-calcifediol/ and https://nutritionmatters.substack.com/p/calcifediol-to-boost-25-hydroxyvitamin .
Why don't we have high dose Cholecalciferol in powder/granule form in Australia? I have been severely deficient in vit-D (below the lowest threshold detectable). In the past, taking 60,000 IU a week (powdered form) for three-six months is what brought my vit-D to detectable levels. I'm not obese. I'm actually underweight. I do not tolerate the oily capsules or the lanoliin based drops (GORD & Gastroparesis). These are the only types of vit-D available to us in Australia. So I have not taken any vit-D at all for 2 years. I think I am screwed. Why are these high dose supplements not permitted in Australia?
The authorities clearly don't give a damn about the "vulnerable", do they? No money in actually saving lives.
#NotAboutHealth