Do lockdowns and border closures serve the “greater good”? A cost-benefit analysis
the COVID lockdowns of this era, can be seen as mass sacrificial event...what did we get in return?

One of the FaceBook posts flagged by the anonymous thought police.
Big Pharma, politicians and public health officers continue to assert that “benefits exceed risks” from the actions of the last 2 years … but none have done anything close to a valid cost-benefit analysis (CBA).
As Gigi states: CBA’s are about welfare, not money.
In this excellent draft document, (which Prof Foster pointed to in her recent appearance on ABC TV’s Q & A Program), when analysed in a Cost-Benefit Analysis context which includes terms such as QALYS ( Quality Adjusted Life Years) and the newer WELLBY ( WellBeing Year), what did we actually get for all those billions of $AUD?
The link to the original, without my highlights and including the references is found here:
https://www.thegreatcovidpanic.com/_files/ugd/23eb94_920d5ddd484640ee8dfca8f045b14886.pdf
Gigi Foster
Professor of Economics, UNSW Business School, University of New South Wales, Sydney, Australia
with Sanjeev Sabhlok
In the past six months we have witnessed a mass worldwide sacrificial event driven by a fear of the unknown and essentially an abandonment of post-Enlightenment thinking. We have been swept up in hysteria and the fanaticism of crowds. Our economy has been stabbed in the stomach.
– Testimony of Gigi Foster to the PAEC, Victoria, August 2020
Since lockdowns are now known to have had no clear beneficial effect on the number of Covid cases or deaths, there is no trade-off to be analysed in the area of lockdown policies. There is just loss all around.
– Paul Frijters et. al. in The Great Covid Panic
There is no doubt in my mind, that when we come to look back on this, the damage done by lockdown[s] will exceed any saving of lives by a huge factor.
– Michael Levitt, Nobel Prize winner in Chemistry
It is possible that lockdown[s] will go down as one of the greatest peacetime policy failures in modern history.
– Douglas Allen, Professor of Economics at Simon Fraser University
SUMMARY OF COSTS AND BENEFITS AND CONCLUSION
Rational public policymaking considers both sides of any proposed policy: benefits and costs. When the costs of lockdown policy have been raised during the COVID era, people have sometimes assumed that those costs are about: “just the economy”, implying that “the economy” is something separable from human health. Yet there are real health and longevity costs of lockdowns, apart from their impacts on the quality of life and overall wellbeing.
In the first half of 2020, the costs of locking down economies should have been weighed against the projected benefits. Best guesses needed to be made about the areas of human wellbeing directly and indirectly affected by lockdown policies. Among other things, we needed to consider the loss of happiness due to loneliness from social isolation, the crowding-out of healthcare for problems other than COVID, the long-term costs to our children and university students of disrupted education, and the economic losses of shuttered businesses, increased inequality, and crowded-out government spending in future years.
In August 2020, I prepared a draft cost-benefit analysis (CBA) for consideration by the Victorian State Parliament1 that was an illustration of how such an exercise could be conducted by the government, whose responsibility it was to provide a rational justification for lockdown policies.
This report updates my outline CBA of August 2020. It includes more context about the methods and about how to approach the robust policy deliberation process that Australian governments should have undertaken early in 2020, and it is structured like a standard CBA except that I do not analyse multiple options. I consider only one: the actual policies adopted in Australia. The alternative that I consider – the benchmark against which the impact of lockdowns is compared – is for the government to have put in place policies that delivered outcomes similar to what Sweden or other “low-restrictions” countries experienced.
Sourcing the data needed for such a process continues to be a challenge, but this is not new. This is a challenge that economists are trained to meet: we try, using the best data available, to come up with reasonable estimates. It would have been nice, for example, to have access to reliable and up-to-date Australian data about various aspects of human wellbeing and suffering. While tools like ANUPoll are useful, we need to build even better tools for analysis of human welfare in Australia. Using conservative assumptions on many different categories of costs and generous assumptions about the benefits of lockdowns, I have pieced together an estimate.
It is in Australia’s interests to provide access to better quality data about its people, activities, and society, so that we can learn more about how to protect and promote welfare. To achieve this, Australia’s departments and research institutions must develop more robust, up-to-date, and relevant data sources and make them available not only to policymakers with a duty to evaluate their policies, but also to independent researchers and the broader public.
I would like to thank Paul Frijters and Michael Baker for their comments on early drafts of this document. Their input greatly helped me to refine the structure and assumptions used.
My deepest heartfelt gratitude goes to Sanjeev Sabhlok, who drew together most of the initial content of this document from existing sources, added and adjusted content diligently at my request, and has been a tireless supporter of the endeavour.
I use the terms COVID and COVID-19 interchangeably in this document. I do not, however, revise the usage in published sources. The disease is increasingly being shortened in the literature to simply “covid.”
Gigi Foster
Sydney, 11 May 2022
1. Executive Summary
The world has been shaken by the response of governments to the COVID-19 pandemic in a way unlike what we have seen in any prior global health event. What started as a local health anomaly in one Chinese province quickly became a world-stopping crisis affecting every major nation in 2020. Industries from travel to manufacturing suffered sudden, acute disruptions due to political action to lock down cities and block free movement of people and goods between countries. Was all of this necessary to save lives, or did it on net produce human damage?
This report aims to evaluate whether Australia’s COVID lockdown policies – a central feature of our COVID policy response – were on net helpful or harmful.
The report is divided into two parts, of which the first is a background discussion that contextualises the analysis, and the second part estimates the costs and benefits of the Australian COVID lockdowns.
1.1 Part 1: Background
I start by discussing the characteristics of good policy processes and summarising the information known early in 2020 that was relevant to responding to COVID. The magnitude of the pandemic is also discussed by reference to history.
1.1.1 What was known pre-COVID
On 24 January 2020, at the beginning of the Wuhan lockdowns, Gauden Galea – the WHO’s representative in China – said that “trying to contain a city of 11 million people is new to science. The lockdown of 11 million people is unprecedented in public health history, so it is certainly not a recommendation the WHO has made.”
This statement summarises the WHO’s known position on the wisdom of lockdowns in 2019, including its official guidance on managing flu-like pandemics, and was also reflected in official policy positions of the developed world before the arrival of COVID-19.
Years before COVID’s arrival, the late Donald Henderson, a major figure in epidemiology who was instrumental in eradicating smallpox from the planet, opined that it is impossible to stop most viruses through border control.
Henderson contended that the spread of most viruses cannot be stopped unless the first case (the “index case”) in a country is stopped, and the next case is stopped, and every additional case is stopped as it erupts. He noted that some viruses can indeed be controlled through quarantines of the sick, and successful attempts have been made to do so (e.g., for Ebola). For most viruses, including the flu, he argued that if even a single person who may not have obvious symptoms slips through the net of control, then the battle is lost.
It is far more sensible in such cases, Henderson argued, not to implement hard border controls but rather to manage the disease in order to minimise harm. In his words: “this idea that in this day and age one is going to intercept people coming across the border and you’re going to stop the spread of the disease is a concept that was antiquated a very long time ago.”
Extended lockdowns of whole populations had never been used in the history of pre-COVID disease control and were regarded as unwise by eminent epidemiological experts such as Donald Henderson. They were known to cause significant negative effects on many other dimensions of society, including our ability to continue to control the target disease.5
Further, counterintuitive though it may seem, there are arguably great public health benefits from human inter-mingling. Some of these may derive directly from our interaction with pathogens, including when we travel internationally. Since at least her “Princeton in Europe” lecture of 2013, Dr Sunetra Gupta of Oxford University has argued that global immunity to viruses is strengthened from international travel:
Virulent pathogens cannot be the only things we bring back from countries where they’ve originated. It is more likely that we’re constantly importing less virulent forms which go undetected because they’re asymptomatic and these may well have the effect of attenuating the severity of infection with their more virulent cousins.
After all the oldest trick up our sleeves is, as vaccination goes, is to use a milder species to protect against a more virulent species. Perhaps this is something we’re inadvertently achieving by mixing more widely with a variety of international pathogens.
According to Dr Gupta, the same principle that applies to children, who “benefit from being exposed to this (COVID) and other seasonal coronaviruses.”7 The logic is that getting a less harmful infection protects children against more serious infections in the future. Therefore, Dr Gupta contends, “the best way to [safeguard against pandemics] is to build up a global wall of immunity. And it may be that we’re unwittingly achieving this through our current patterns of international travel.” As part of our response to COVID-19, we have paused this potential mechanism of building group-level immunity to pathogens.
The World Health Organization’s position on pandemic management prior to COVID-19 included recommending some voluntary preventative measures for a virus like COVID, such as handwashing and avoiding crowds, but no border closures and quarantines, and no mandated restrictions on the movement of healthy people under any circumstances. If such restrictions had been favoured by pre-COVID scientific consensus, this would have been reflected in many scientific contributions prior to 2020 advocating policies like lockdowns after evaluating their costs and benefits. In fact, to my knowledge, virtually no scholarly works published after WWII and prior to 2020 argue that restrictions on the movements of healthy populations would result or ever have resulted in positive net benefits in terms of human welfare, wellbeing, or lives.9
1.1.2 COVID in historical context
A key element of contextualising a cost-benefit analysis of any policy is to understand the magnitude of the problem that the policy purports to address. It has been known since early 2020 that the threat posed by COVID is not severe by historical or pathogenic comparison. Victoria’s pandemic plan of 10 March 2020 indicated that the original strain of “COVID-19 is assessed as being of moderate clinical severity.” It has also been clear since then that COVID is largely a non-event in children but can be severe in the elderly and those with comorbidities.
There were 50 million global deaths in 1918-1919 from the Spanish flu when the world’s population was 1.8 billion. The current world population is 7.9 billion, meaning that around 219 million people would need to die of COVID if the COVID pandemic were in the league of the Spanish flu in terms of raw numbers of deaths. As displayed in Figure 1.1, there have been about 7 million deaths with COVID reported by Worldometer10 to date, or more than 30 times fewer than 219 million.
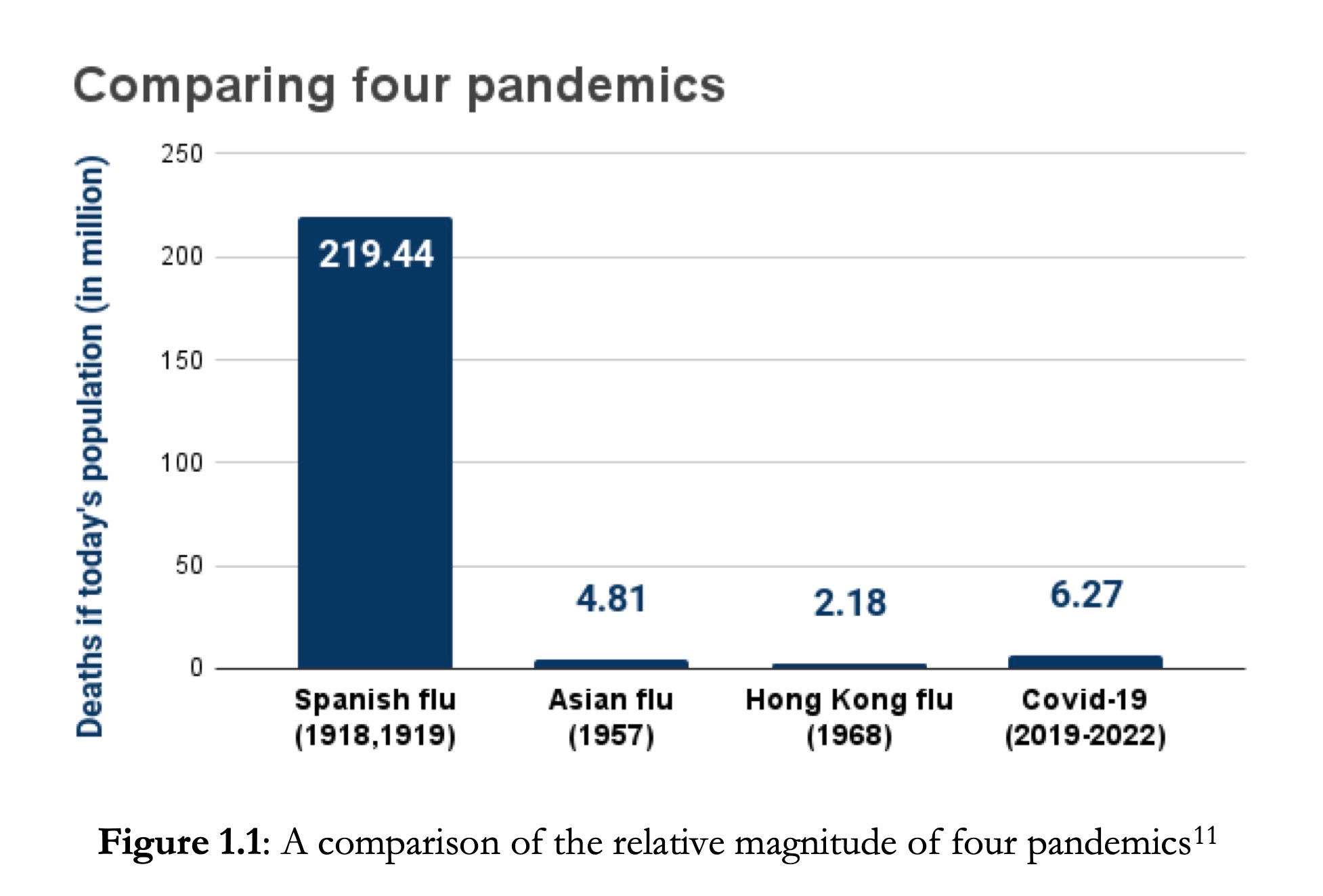
Figure 1.1: A comparison of the relative magnitude of four pandemics
On 9 April 2022, John Ioannidis of Stanford, one of the world’s most highly citied epidemiologists today, wrote to Sanjeev Sabhlok: “You are correct, the 1918 flu was 50-500 times worse than COVID-19 once you adjust for population size and for age distribution. I have highlighted this recently in a paper on the end of the pandemic that includes a detailed table comparing the impact of pandemics versus the seasonal flu. Deaths from SARS-CoV-2 COVID-19 was just 1.5-4 times the equivalent of three seasons of seasonal flu (most likely closer to the 1.5 number actually). Spanish flu was 100-1000 times bigger than 3 seasons of seasonal flu. https://onlinelibrary.wiley.com/doi/10.1111/eci.13782”.12 Augmenting this conclusion is that fact that since the Spanish flu severely impacted the young, while COVID’s victims are mainly elderly, the Spanish flu was even more lethal in terms of potential life years lost.
Even if the many legitimate questions about COVID death reporting are ignored, the severity of the COVID pandemic is in the range of the Asian flu of 1957 (also shown in Figure 1.1), in response to which healthy populations were not locked down.
1.1.3 Providing a cost-benefit analysis is the responsibility of the government
It is incumbent upon a democratic government pursuing sound policy-making principles to conduct and provide for public examination a cost-benefit analysis of major policies that transparently estimates and weighs all known or expected benefits and all known or expected harms. No such analysis has been forthcoming in Australia to provide a justification for the COVID lockdowns, despite such a requirement being deeply embedded in the standard policy processes of Australia.
On 12 August 2020, in light of the government’s failure to discharge its responsibility in this regard, I presented a preliminary cost-benefit analysis of Victoria’s lockdowns to the Public Accounts and Estimates Committee of Victoria’s State Parliament.13 My analysis was intended as a demonstration of approach and offered a generous estimate of the benefits and only a partial accounting of the costs of lockdowns. I noted that a comprehensive cost-benefit analysis would need to factor in a wide variety of additional costs, many of which I enumerated but did not fully cost out in the document.
No level of Australian government has yet provided a CBA justifying COVID lockdowns. The present report expands my August 2020 draft CBA by providing estimates for more cost and benefit categories, and updates it to cover the costs and plausible benefits of COVID lockdown policies implemented through the end of 2021.
Part II: The cost-benefit analysis
This expanded CBA confirms that the costs of wholesale lockdowns for Australia are far greater than their benefits in a COVID world, even using the most conservative assumptions in favour of the government’s lockdown policies.
1.2.1 Methodological observations
A few methodological observations are in order.
This CBA is retrospective, not prospective.
A proper policy analysis using a CBA approach considers not just one policy alternative (lockdowns, in this case) but a wide range of options. A scenario analysis is also usually included to accommodate the inevitable uncertainty about projected costs and benefits. Only then is the appropriate policy selected. While this report alludes to a range of potential options that were available to the government at the outset of the pandemic, it is retrospective and looks only at the effects of the actual policies that have been implemented in Australia, relative to a default policy of managing COVID in what would have been considered the best-practice manner before March 2020: i.e., compliance of Australian governments with their own risk-based pandemic plans which preclude wholesale lockdowns or border closures, but include targeted restrictions and voluntary social distancing. Such an approach is proxied in this paper by taking actions that would have delivered outcomes similar to what countries with policy settings like Sweden achieved in 2020 and 2021.
CBAs are about social welfare, not money.
There is a prevalent misconception that CBAs are about money. They are in fact about social welfare. The approach taken in this report considers statistical lives lost now and in the future, and also counts, for example, the mental health suffering that people endure when they are locked inside their homes. In the CBA presented here, the human welfare costs of lockdowns are put into a currency (quality-adjusted life years, or QALYs) that is used to enumerate both projected costs and benefits of the lockdowns. I also use the newly created WELLBY (wellbeing year) measure to capture some lockdown costs. Since one year of average healthy life (1 QALY) equates to 6 WELLBYs experienced by a person for one year, this allows suffering across the society to be compared with benefits in the same welfare “currency.”
A conservative approach is adopted.
Every assumption about the costs of lockdowns that I make in this CBA is supported directly or indirectly by the research literature and evidence. The only assumptions I make that have scant backing are my conservative assumptions in favour of lockdowns, i.e., in favour of trying to find that lockdowns are helpful. I assume that COVID deaths would be avoided by lockdowns, which is an assumption not borne out in other countries’ experiences,15 but arguably true to a small extent in Australia, at least insofar as blocking international travel will have reduced the amount of virus circulating within Australia for a period of time.
Sweden and other countries with mild restrictions serve as counterfactuals.
To estimate the losses avoided by lockdowns, I consider two alternative counterfactuals: the outcomes achieved by Sweden, and those achieved by a set of six nations with low levels of COVID restrictions. In the final analysis I count the higher of these two estimates – using population-adjusted data from Sweden as the counterfactual – to be the upper-end amount of loss potentially avoided because of Australia’s lockdown policies.
Worldometer16 shows that more than 50 countries with harsh lockdowns have experienced more COVID deaths per million than Sweden which had no lockdowns, mandatory masks, quarantines or border closures. If the Worldometer data is adjusted for Sweden’s high latitude (with likely low vitamin D levels), age structure (20% of Sweden’s population is over 65 and hence more vulnerable to the virus, compared with 18.9% in the UK and 9.3% across the world), the “dry tinder” effect (a low mortality rate from flu in the December 2019 through March 2020 flu season in Sweden17 meant that more vulnerable people were around to be attacked by COVID, or other diseases, later in 2020), higher density nursing and aged care homes, and likely over-reporting of COVID deaths in Sweden, then the COVID death rate in Sweden would look even more modest. Hence, the choice to use Sweden as a counterfactual likely yields an over- estimate of the benefits of lockdowns.
1.2.2 Benefits of lockdowns
In this paper I calculate 12,304 deaths as the upper-end estimate for the number of COVID deaths that could have occurred in Australia during 2020 and 2021 without lockdowns. There were in fact 2,353 COVID deaths in Australia in these two years, even in the presence of lockdowns, so at most 9,951 COVID deaths were avoided by lockdown policies.
On average a COVID death represents a loss of 3 to 5 QALYs,19 since on average such a death occurs in someone already significantly advanced in age and not in good health. I use the higher figure of 5 in this report, to be generous to lockdowns.
To this, based on estimates of the incidence and severity of long COVID,20 one can add 2% of the estimated losses in the form of COVID deaths to account for the human cost of long-COVID effects. One can also add an estimated 131 deaths by homicide and traffic accidents, often of significantly younger age than the average COVID victim, that would have occurred in a no-lockdown regime.
We therefore arrive at the following upper-end estimate for the total benefit of lockdowns:
9,951 (total COVID deaths averted) x 5 (healthy years lost per COVID death) x 6 (WELLBYs per QALY) x 1.02 (estimate for long COVID) + 131 (non-COVID deaths averted) x 50 (healthy years lost per each such death) x 6 (WELLBYs per QALY) = 343,800 WELLBYs, or 57,300 QALYs, in all.
Dividing this total by 24 (the number of months in two years), we get approximately 14,325 WELLBYs saved per month of lockdown.
How much would Australian society be willing to pay to avoid this quantity of loss?
Taking a high estimate of AU$100,000 as the amount Australian society would be willing to pay to save one QALY – which is an upper-bound estimate based on what the TGA pays in normal years to buy medical interventions that save QALYs21 – then Australian society would be willing to pay a total of 57,300 (i.e., total QALYs saved) x 100,000 = AU$5.73 billion over the course of two years to avoid this magnitude of loss.
The maximum that Australia would normally be willing to spend to prevent an additional 9,951 COVID deaths plus 131 traffic/homicide deaths – even using very conservative assumptions in favour of the government’s policies – is therefore around six billion dollars.
In fact, hundreds of billions of dollars have been spent. This itself instantly suggests that alternative policy options should have been considered. It is also broadly consistent with the findings of a simple dollars- and-QALYs-based cost-benefit analysis of Australia’s lockdowns published in January 2022 by Martin T. Lally, who finds that at least 11 times more has been spent by the government allegedly to prevent COVID deaths than would have been spent in a normal policy regime, in which Australia would have been willing to spend a maximum of $100,000 per QALY saved.
Have lockdowns avoided 40,000 deaths?
In the lead-up to the election in May 2022, the Prime Minister of Australia is reported to have claimed that 40,000 deaths have been avoided by his “regime” (of lockdowns and border closures).23 Earlier, he had sent letters to many Australians in which he made a slightly more modest claim of having prevented 30,000 deaths.24 No substantiating evidence was provided for these assertions, but it is possible that the Prime Minister used estimates based on epidemiological models.
Even if Mr Morrison’s most extreme claim were correct and 40,000 COVID deaths had been prevented by lockdowns, that would still bound at AU$20 billion the amount Australia would have been willing to pay to pursue the lockdown strategy, using the observation above that Australia is willing to pay at most AU$100,000 per QALY saved. Spending more than that would have diverted scarce resources from other competing priorities that, from a human wellbeing perspective, also matter.
In fact, we have spent hundreds of billions of dollars pursuing lockdowns and cushioning their economic fallout.
1.2.3 Costs of lockdowns
Imposing crippling restrictions on 99% of the population will necessarily cause significant overall harm. Evidence from numerous CBAs undertaken across the world has already indicated, for many countries, that lockdowns are damaging and even that they do not on net save lives. Lockdowns and social-distancing measures inflict unemployment, business collapse, education neglect, health neglect and loneliness. The virus does not do these things; government directives do these things.
1.2.4 Cost-benefit ratio
I estimate the maximum benefits from lockdown policies to be 343,800 WELLBYs, and the minimum costs
from lockdowns to be 12.44 million WELLBYs.
This indicates that the costs of Australia’s COVID lockdowns have been at least 36 times greater than the benefits they delivered.
Since I have made assumptions that are extremely favourable to the government’s choice to pursue a lockdown strategy, the true ratio of costs to benefits of the Australian COVID lockdowns is likely greater than this.
Opportunity costs: Deaths that could have been avoided with dollars spent on COVID
Another way to evaluate the effectiveness of policies to minimise harm from COVID starts with the following question: what is the opportunity cost of the dollars we have spent on our COVID response?
According to the Australian Institute of Health and Welfare:
Potentially avoidable deaths are deaths among people younger than 75 that are potentially avoidable within the present health care system. They include deaths from conditions that are potentially preventable through individualised care and/or treatable through existing primary or hospital care. In 2019, there were 28,000 potentially avoidable deaths: half (48%) of all deaths for people aged less than 75. Of these deaths, 64% were male and 36% were female.
One could estimate quite easily how many lives could have been saved if the hundreds of billions of dollars spent by the government on lockdowns, and policies associated with the disruption they caused, had instead been spent on other health priorities.
Such an exercise leads to the conclusion that if hundreds of billions of dollars had been invested in non-COVID-related health care during 2020 and 2021, instead of being used to pursue lockdowns and cushion their fallout, Australia could have avoided tens of thousands of (non-COVID) deaths. Spending some of this money on early treatment of those infected with COVID would also have saved more lives on net than lockdowns did.
1.4 Limitations of this study
Like any cost-benefit analysis, this document is not definitive. I expect many of the costs imposed by lockdowns, particularly through the unintended consequences of these policies, to become clearer and more measurable over time. Individual line items will need to be updated, but more broadly, future researchers bear the responsibility to attempt the difficult task of valuing the intangible costs of the Australian lockdowns to Australians’ stance towards their government and society. Such costs arise from the loss of individual liberty, the fracture of communities, and the abandonment of principles of good governance and public health stewardship as our governments became propagandists. I hope that future research will deliver estimates of the cost of the marginal changes to trust and belief in government, in our institutions (including public health), and in one another, that lockdowns have wrought.
While the list of costs is expected to expand with time, few new benefits of lockdowns are likely to emerge. This is because the plausible benefits of lockdowns, and those on the basis of which they were originally defended, are mainly those occurring in the short run (i.e., during the lockdowns themselves). Consequently, I do not expect my conclusion that net damage was done to Australia by lockdowns to be reversed by future information. I suspect, instead, that the adverse assessment of lockdowns illustrated in this CBA is likely to worsen. I have characterised the COVID lockdowns of this era as a mass sacrificial event, and I sadly expect future data and future research merely to re-confirm this assessment.